Abhijith, K. V., et al., 2017, ‘Air pollution abatement performances of green infrastructure in open road and built-up street canyon environments — a review’, Atmospheric Environment 162, pp. 71-86 (DOI: 10.1016/j.atmosenv.2017.05.014).
Aguilar, A. J., et al., 2022, ‘Assessment of ventilation rates inside educational buildings in Southwestern Europe: analysis of implemented strategic measures’, Journal of Building Engineering 51, 104204 (DOI: 10.1016/j.jobe.2022.104204).
An, F., et al., 2021, ‘A review of the effect of traffic-related air pollution around schools on student health and its mitigation’, Journal of Transport & Health 23, 101249 (DOI: 10.1016/j.jth.2021.101249).
Baldauf, R., et al., 2015, Best practices for reducing near-road pollution exposure at schools, United States Environmental Protection Agency (https://19january2017snapshot.epa.gov/sites/production/files/2015-10/documents/ochp_2015_near_road_pollution_booklet_v16_508.pdf) accessed 5 April 2023.
Beregszaszi, T., et al., 2013, School environment and respiratory health of children making schools healthy: meeting environment and health challenges, SEARCH Initiative (DOI: 10.13140/2.1.4525.4089).
Bettiol, A., et al., 2021, ‘The first 1000 days of life: traffic-related air pollution and development of wheezing and asthma in childhood. A systematic review of birth cohort studies’, Environmental Health 20(1), 46 (DOI: 10.1186/s12940-021-00728-9).
Blaakman, S., et al., 2013, ‘Implementation of a community-based secondhand smoke reduction intervention for caregivers of urban children with asthma: process evaluation, successes and challenges’, Health Education Research 28(1), pp. 141-152 (DOI: 10.1093/her/cys070).
Boniardi, L., et al., 2021, ‘Personal exposure to equivalent black carbon in children in Milan, Italy: time-activity patterns and predictors by season’, Environmental Pollution 274, 116530 (DOI: 10.1016/j.envpol.2021.116530).
Bowatte, G., et al., 2018, ‘Air pollution and otitis media in children: a systematic review of literature’, International Journal of Environmental Research and Public Health 15(2), 257 (DOI: 10.3390/ijerph15020257).
Brand, E., et al., 2019, Kennisoverzicht vraagstukken diffuus lood in de bodem, RIVM Rapport 2019-0006, Rijksinstituut voor Volksgezondheid en Milieu (DOI: 10.21945/RIVM-2019-0006).
Bunik, M., et al., 2013, ‘The ONE Step Initiative: quality improvement in a pediatric clinic for secondhand smoke reduction’, Pediatrics 132(2), pp. e502-e511 (DOI: 10.1542/peds.2011-1271).
Burkhardt, T., et al., 2023, ‘Time trend of exposure to secondhand tobacco smoke and polycyclic aromatic hydrocarbons between 1995 and 2019 in Germany — showcases for successful European legislation’, Environmental Research 216(Pt 2), 114638 (DOI: 10.1016/j.envres.2022.114638).
Burns, J., et al., 2020, ‘Interventions to reduce ambient air pollution and their effects on health: an abridged Cochrane systematic review’, Environment International 135, 105400 (DOI: 10.1016/j.envint.2019.105400).
Caldwell, A. L., et al., 2018, ‘Parental smoking cessation: impacting children’s tobacco smoke exposure in the home’, Pediatrics 141(Suppl 1), pp. S96-S106 (DOI: 10.1542/peds.2017-1026M).
Carreras, G., et al., 2019, ‘Burden of disease attributable to second-hand smoke exposure: a systematic review’, Preventive Medicine 129, 105833 (DOI: 10.1016/j.ypmed.2019.105833).
Carreras, G., et al., 2020, ‘Burden of disease from breast cancer attributable to smoking and second-hand smoke exposure in Europe’, International Journal of Cancer 147(9), pp. 2387-2393 (DOI: 10.1002/ijc.33021).
Chen, Z., et al., 2015, ‘Chronic effects of air pollution on respiratory health in Southern California children: findings from the Southern California Children’s Health Study’, Journal of Thoracic Disease 7(1), pp. 46-58 (DOI: 10.3978/j.issn.2072-1439.2014.12.20).
Chillón, P., et al., 2015, ‘A longitudinal study of the distance that young people walk to school’, Health & Place 31, pp. 133-137 (DOI: 10.1016/j.healthplace.2014.10.013).
Collins, B. N., et al., 2015, ‘Reducing underserved children’s exposure to tobacco smoke’, American Journal of Preventive Medicine 49(4), pp. 534-544 (DOI: 10.1016/j.amepre.2015.03.008).
Collins, B. N., et al., 2018, ‘An office-initiated multilevel intervention for tobacco smoke exposure: a randomized trial’, Pediatrics 141(Suppl 1), pp. S75-S86 (DOI: 10.1542/peds.2017-1026K).
Collins, B. N., et al., 2020, ‘Long-term results from the FRESH RCT: sustained reduction of children’s tobacco smoke exposure’, American Journal of Preventive Medicine 58(1), pp. 21-30 (DOI: 10.1016/j.amepre.2019.08.021).
Davis, A., 2020, School street closure and traffic displacement: a literature review and semi-structured interviews, Transport Research Institute, Edinburgh Napier University, Edinburgh, UK.
de Nazelle, A., et al., 2017, ‘Comparison of air pollution exposures in active vs. passive travel modes in European cities: a quantitative review’, Environment International 99, pp. 151-160 (DOI: 10.1016/j.envint.2016.12.023).
Den Hond, E. et al., 2020, Interventiestudie schoolomgeving: impact van schoolstraat, samenvatting, VITO-AZG rapport (https://www.zorg-en-gezondheid.be/sites/default/files/2022-04/Studie%20impact%20schoolstraat%20-%20Samenvatting%20algemene%20publiek.pdf) accessed 5 April 2023 (only available in Dutch).
Dick, S., et al., 2014, ‘Associations between environmental exposures and asthma control and exacerbations in young children: a systematic review’, BMJ Open 4(2), e003827 (DOI: 10.1136/bmjopen-2013-003827).
Dirks, K. N., et al., 2016, ‘Air pollution exposure in relation to the commute to school: a Bradford UK case study’, International Journal of Environmental Research and Public Health 13(11), 1064 (DOI: 10.3390/ijerph13111064).
Dutheil, F., et al., 2021, ‘Autism spectrum disorder and air pollution: a systematic review and meta-analysis’, Environmental Pollution 278, 116856 (DOI: 10.1016/j.envpol.2021.116856).
EEA, 2021, Air quality management, EEA Briefing, European Environment Agency (https://www.eea.europa.eu/themes/air/air-quality-management) accessed 5 April 2023.
EEA, 2022a, Air quality in Europe 2022, EEA Web Report, European Environment Agency (https://www.eea.europa.eu/publications/air-quality-in-europe-2022) accessed 30 November 2022.
EEA, 2022b, Sources and emissions of air pollutants in Europe, EEA Web Report, European Environment Agency (https://www.eea.europa.eu/publications/air-quality-in-europe-2021/sources-and-emissions-of-air) accessed 24 October 2022.
EEA, 2022c, Zero pollution monitoring assessment, EEA Web Report No 3/2022, European Environment Agency (https://www.eea.europa.eu/publications/zero-pollution) accessed 8 December 2022.
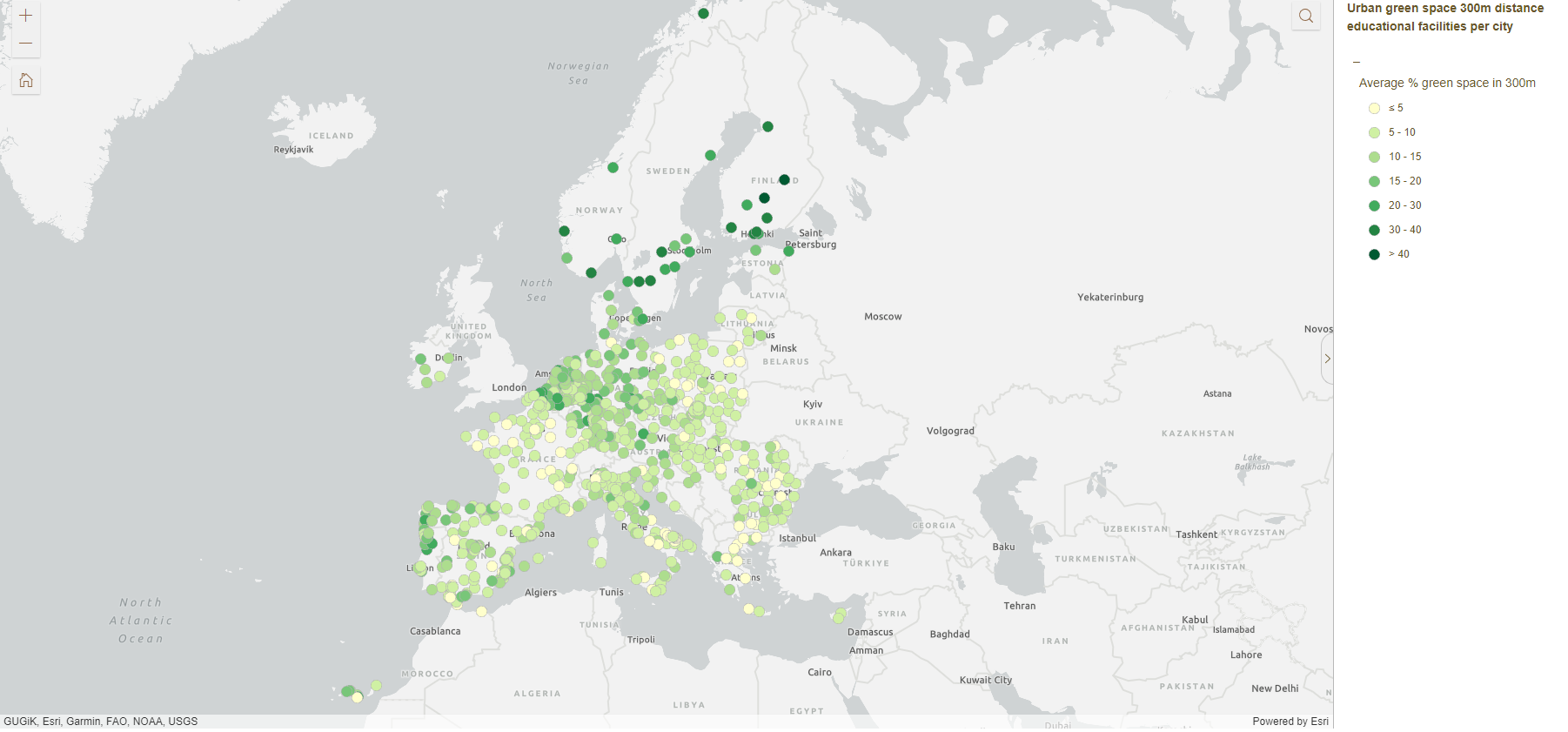
EEA, 2023, ‘Average percentage of urban green space withing 300m distance of educational facilities in European cities, 2020’ European Climate and Health Observatory’, European Environment Agency (https://sdi.eea.europa.eu/catalogue/climate-health/eng/catalog.search#/metadata/222b657f-de55-4cbf-b2ab-acc961c49dbc) accessed 5 April 2023.
El Sharkawy, M., et al., 2021, ‘Change in exposure of children to second-hand smoke with impact on children’s health and change in parental smoking habits after smoking ban in Bavaria — a multiple cross-sectional study’, BMC Public Health 21(1), 2134 (DOI: 10.1186/s12889-021-12130-8).
EU, 2004, Directive 2004/107/EC of the European Parliament and of the Council of 15 December 2004 relating to arsenic, cadmium, mercury, nickel and polycyclic aromatic hydrocarbons in ambient air (OJ L 23, 26.1.2005, p. 3-16).
EU, 2008, Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe (OJ L 152, 11.6.2008, p. 1-44).
EU, 2016, Directive 2016/2284/EC of the European Parliament and of the Council of 14 December 2016 on the reduction of national emissions of certain atmospheric pollutants, amending Directive 2003/35/EC and repealing Directive 2001/81/EC (OJ L 344, 17.12.2016, p. 1-31).
European Commission, et al., 2014, SINPHONIE: Schools Indoor Pollution & Health Observatory Network in Europe: final report, Publications Office of the European Union, Luxembourg.
European Commission, 2020, Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the regions ‘Chemicals Strategy for Sustainability Towards a Toxic-Free Environment’ (https://eur-lex.europa.eu/resource.html?uri=cellar:f815479a-0f01-11eb-bc07-01aa75ed71a1.0003.02/DOC_1&format=PDF) accessed 5 April 2023.
European Commission, 2021, ‘Statement by President von der Leyen on delivering the European Green Deal’ (https://ec.europa.eu/commission/presscorner/detail/en/statement_21_3701) accessed 5 April 2023.
European Commission, 2022a, ‘Air quality — existing legislation’ (https://ec.europa.eu/environment/air/quality/existing_leg.htm) accessed 5 April 2023.
European Commission, 2022b, ‘Zero pollution action plan’ (https://ec.europa.eu/environment/strategy/zero-pollution-action-plan_en) accessed 5 April 2023.
Eurostat, 2019, ‘More than 95% of children in the EU considered to be in good or very good health’ (https://ec.europa.eu/eurostat/documents/2995521/9550240/3-05022019-BP-EN.pdf/f426eec4-bbff-48f0-8084-88d721fa49ef#:~:text=In%202017%2C%20more%20than%2095,those%20aged%20ten%20to%20fifteen.) accessed 5 April 2023.
Fairburn, J., et al., 2019, ‘Social inequalities in exposure to ambient air pollution: a systematic review in the WHO European Region’, International Journal of Environmental Research and Public Health 16(17) (DOI: 10.3390/ijerph16173127).
Fakunle, A. G., et al., 2020, ‘Indoor microbiome and risk of lower respiratory tract infections among children under-five years: a meta-analysis’, Indoor Air 30(5), pp. 795-804 (DOI: 10.1111/ina.12698).
Fakunle, A. G., et al., 2021, ‘Association of indoor microbial aerosols with respiratory symptoms among under-five children: a systematic review and meta-analysis’, Environmental Health 20(1), 77 (DOI: 10.1186/s12940-021-00759-2).
Filippini, T., et al., 2019, ‘Association between outdoor air pollution and childhood leukemia: a systematic review and dose-response meta-analysis’, Environmental Health Perspectives 127(4), 46002 (DOI: 10.1289/ehp4381).
Fisk, W. J., 2017, ‘The ventilation problem in schools: literature review’, Indoor Air 27(6), pp. 1039-1051 (DOI: 10.1111/ina.12403).
Garcia, E., et al., 2021, ‘Air pollution and lung function in children’, Journal of Allergy and Clinical Immunology 148(1), pp. 1-14 (DOI: c).
GBD Collaborative Network, 2020, ‘GBD Results’, Institute for Health Metrics and Evaluation (http://ghdx.healthdata.org/gbd-results-tool) accessed 5 April 2023.
Gern, J. E., et al., 1999, ‘Early life origins of asthma’, Journal of Clinical Investigation 104(7), pp. 837-843 (DOI: 10.1172/JCI8272).
Ghosh, R., et al., 2021, ‘Ambient and household PM2.5 pollution and adverse perinatal outcomes: a meta-regression and analysis of attributable global burden for 204 countries and territories’, PLoS Med 18(9), e1003718 (DOI: 10.1371/journal.pmed.1003718).
Gouvernement de France, 2022, ‘Qualité de l’air intérieur’, Ministères Écologie Énergie Territoires (https://www.ecologie.gouv.fr/qualite-lair-interieur) accessed 16 August 2022.
Grippo, A., et al., 2018, ‘Air pollution exposure during pregnancy and spontaneous abortion and stillbirth’, Review of Environmental Health 33(3), pp. 247-264 (DOI: 10.1515/reveh-2017-0033).
Han, K., et al., 2021, ‘Traffic-related organic and inorganic air pollution and risk of development of childhood asthma: a meta-analysis’, Environmental Research 194, 110493 (DOI: 10.1016/j.envres.2020.110493).
Hänninen, O., et al., 2011, European perspectives on environmental burden of disease estimates for nine stressors in six European countries, THL Report No 01/2011, National Institute for Health and Welfare, Helsinki.
Health Effects Institute, 2022, Systematic review and meta-analysis of selected health effects of long-term exposure to traffic-related air pollution, Special Report 23, Health Effects Institute, Boston, MA (https://www.healtheffects.org/system/files/traffic-press-release-final2.pdf) accessed 22 June 2022.
Hoehn, J. L., et al., 2016, ‘Barriers and motivators to reducing secondhand smoke exposure in African American families of head start children: a qualitative study’, Health Education Research 31(4), pp. 450-464 (DOI: 10.1093/her/cyw028).
Holm, S. M. and Balmes, J. R., 2022, ‘Systematic review of ozone effects on human lung function, 2013 through 2020’, Chest 161(1), pp. 190-201 (DOI: 10.1016/j.chest.2021.07.2170).
Huang, J., et al., 2021, ‘Outdoor air pollution and the risk of asthma exacerbations in single lag0 and lag1 exposure patterns: a systematic review and meta-analysis’, Journal of Asthma, 59(11), pp. 2322-2339 (DOI: 10.1080/02770903.2021.2008429).
Huertas-Delgado, F. J., et al., 2022, ‘Associations between parental reasons for choosing a neighborhood and adolescents’ physical activity and commuting behaviors’, Journal of Transport & Health 24, 101259 (DOI: 10.1016/j.jth.2021.101259).
Hurraß, J., et al., 2017, ‘Medical diagnostics for indoor mold exposure’, International Journal of Hygiene and Environmental Health 220(2 Pt B), pp. 305-328 (DOI: 10.1016/j.ijheh.2016.11.012).
Jhun, I., et al., 2017, ‘School environmental intervention to reduce particulate pollutant exposures for children with asthma’, Journal of Allergy and Clinical Immunology: In Practice 5(1), pp. 154-159 (DOI: 10.1016/j.jaip.2016.07.018).
Kanchongkittiphon, W., et al., 2015, ‘Indoor environmental exposures and exacerbation of asthma: an update to the 2000 review by the Institute of Medicine’, Environmental Health Perspectives 123(1), pp. 6-20 (DOI: 10.1289/ehp.1307922).
King, C., et al., 2018, ‘The effect of outdoor air pollution on the risk of hospitalisation for bronchiolitis in infants: a systematic review’, Peer J6 (DOI: 10.7717/peerj.5352).
Koppen et al., 2020,Interventiestudie schoolomgeving: impact van schoolstraat, deelrapport 5 – gezondheidsmetingen, VITO-AZG rapport (https://www.zorg-en-gezondheid.be/studies-en-rapporten-gezonde-publieke-ruimte#6) accessed 5 April 2023 (only available in Dutch).
Kumar, P. et al., 2020,Mitigating exposure to traffic pollution in and around schools. Guidance for children, schools and local communities (DOI: https://doi.org/10.5281/zenodo.3754131).
Kuntz, B. and Lampert, T., 2016, ‘Tabakkonsum und Passivrauchbelastung bei Jugendlichen in Deutschland’, Deutsches Arzteblatt International 113(3), pp. 23-30 (DOI: 10.3238/arztebl.2016.0023).
Låg, M., et al., 2020, ‘Potential role of polycyclic aromatic hydrocarbons in air pollution-induced non-malignant respiratory diseases’, Respiratory Research 21(1), 299 (DOI: 10.1186/s12931-020-01563-1).
Laverty, A. A., et al., 2021, ‘Smoke-free vehicles: impact of legislation on child smoke exposure across three countries’, European Respiratory Journal 58(6), 2004600 (DOI: 10.1183/13993003.04600-2020).
Lee, S. Y., et al., 2020, ‘Associations between particulate matter and otitis media in children: a meta-analysis’, International Journal of Environmental Research and Public Health 17(12), 4604 (DOI: 10.3390/ijerph17124604).
Liang, L. A., et al., 2016, ‘Children’s exposure to second-hand smoke before and after the smoking ban in Bavaria — a multiple cross-sectional study’, European Journal of Public Health 26(6), pp. 969-974 (DOI: 10.1093/eurpub/ckw099).
Lim, H., et al., 2016, ‘Short-term effect of fine particulate matter on children’s hospital admissions and emergency department visits for asthma: a systematic review and meta-analysis’, Journal of Preventive Medicine and Public Health 49(4), pp. 205-219 (DOI: 10.3961/jpmph.16.037).
Lin, L. Z., et al., 2022, ‘The epidemiological evidence linking exposure to ambient particulate matter with neurodevelopmental disorders: a systematic review and meta-analysis’, Environmental Research 209, 112876 (DOI: 10.1016/j.envres.2022.112876).
Lowther, S. D., et al., 2021, ‘Low level carbon dioxide indoors — a pollution indicator or a pollutant? A health-based perspective’, Environments 8(11), 125 (DOI: 10.3390/environments8110125).
Mason, M. J., et al., 2016, ‘The dynamic role of urban neighborhood effects in a text-messaging adolescent smoking intervention’, Nicotine & Tobacco Research 18(5), pp. 1039-1045 (DOI: 10.1093/ntr/ntv254).
Mehta, S., et al., 2013, ‘Ambient particulate air pollution and acute lower respiratory infections: a systematic review and implications for estimating the global burden of disease’, Air Quality, Atmosphere & Health 6(1), pp. 69-83 (DOI: 10.1007/s11869-011-0146-3).
Mendoza, D. L., et al., 2022, ‘Air quality and behavioral impacts of anti-idling campaigns in school drop-off zones’, Atmosphere 13(5), 706 (DOI: 10.3390/atmos13050706).
Mustafić, H., et al., 2012, ‘Main air pollutants and myocardial infarction: a systematic review and meta-analysis’, JAMA 307(7), pp. 713-721 (DOI: 10.1001/jama.2012.126).
Nhung, N. T. T., et al., 2017, ‘Short-term association between ambient air pollution and pneumonia in children: a systematic review and meta-analysis of time-series and case-crossover studies’, Environmental Pollution 230, pp. 1000-1008 (DOI: 10.1016/j.envpol.2017.07.063).
NICE, 2017, ‘Air pollution: outdoor air quality and health’ National Institute for Health and Care Excellence (https://www.nice.org.uk/guidance/ng70) accessed 2 November 2022.
Nogueira, S. O., et al., 2022, ‘Secondhand smoke exposure in European countries with different smoke-free legislation: findings from the EUREST-PLUS ITC Europe surveys’, Nicotine & Tobacco Research 24(1), pp. 85-92 (DOI: 10.1093/ntr/ntab157).
Nyadanu, S. D., et al., 2022, ‘Prenatal exposure to ambient air pollution and adverse birth outcomes: an umbrella review of 36 systematic reviews and meta-analyses’, Environmental Pollution306, 119465 (DOI: 10.1016/j.envpol.2022.119465).
Öberg, M., et al., 2010, Second-hand smoke: assessing the burden of disease at national and local levels, Environmental Burden of Disease Series, World Health Organization, Geneva.
Öberg, M., et al., 2011, ‘Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries’, The Lancet 377(9760), pp. 139-146 (DOI: 10.1016/S0140-6736(10)61388-8).
Orsini, N., et al., 2012, ‘Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software’, American Journal of Epidemiology 175(1), pp. 66-73 (DOI: 10.1093/aje/kwr265).
Osborne, S., et al., 2021, ‘Air quality around schools: Part I — A comprehensive literature review across high-income countries’, Environmental Research 196, 110817 (DOI: 10.1016/j.envres.2021.110817).
Van Poppel et al., 2021, Studie naar het effect van een schoolstraat op de luchtkwaliteit, (https://www.zorg-en-gezondheid.be/studies-en-rapporten-gezonde-publieke-ruimte#6). Accessed 5 April 2023.
Public Health England, 2019,Review of interventions to improve outdoor air quality and public health, Public Health England, London, UK.
Pun, V. C., et al., 2021, ‘Ambient and household air pollution on early-life determinants of stunting — a systematic review and meta-analysis’, Environmental Science and Pollution Research International 28(21), pp. 26404-26412 (DOI: 10.1007/s11356-021-13719-7).
Rafiepourgatabi, M., et al., 2021, ‘The effect of route choice in children’s exposure to ultrafine particles whilst walking to school’, International Journal of Environmental Research and Public Health 18(15), 7808 (DOI: 10.3390/ijerph18157808).
Redondo-Bermúdez, M. del C., et al., 2022, ‘Green infrastructure for air quality plus (GI4AQ+): defining critical dimensions for implementation in schools and the meaning of “plus” in a UK context’, Nature-Based Solutions 2, 100017 (DOI: 10.1016/j.nbsj.2022.100017).
Rijkswaterstaat Environment, 2022, ‘Dutch policy and regulations for air quality’ (https://rwsenvironment.eu/subjects/air/air-quality/) accessed 2 November 2022.
Rivas, I., et al., 2018, ‘How to protect school children from the neurodevelopmental harms of air pollution by interventions in the school environment in the urban context’, Environment International 121, pp. 199-206 (DOI: 10.1016/j.envint.2018.08.063).
Rojas-Rueda, D., et al., 2019, ‘Environmental burden of childhood disease in Europe’, International Journal of Environmental Research and Public Health 16(6), 1084 (DOI: 10.3390/ijerph16061084).
Rumchev, K., et al., 2021, ‘Reducing car idling at primary schools: an intervention study of parent behaviour change in Perth, Western Australia’, Health Promotion Journal of Australia 32(3), pp. 383-390 (DOI: 10.1002/hpja.381).
Ryan, P. H., et al., 2013, ‘The impact of an anti-idling campaign on outdoor air quality at four urban schools’, Environmental Science: Processes & Impacts 15(11), pp. 2030-2037 (DOI: 10.1039/c3em00377a).
Selroos, O., et al., 2015, ‘National and regional asthma programmes in Europe’, European Respiratory Review 24(137), pp. 474-483 (DOI: 10.1183/16000617.00008114).
Senatsverwaltung für Umwelt, Mobilität, Verbraucher- und Klimaschutz, 2022, ‘Luftqualität’ (https://www.berlin.de/sen/uvk/umwelt/luft/luftqualitaet/) accessed 2 November 2022.
Sharifi, M., et al., 2014, ‘Enhancing the electronic health record to increase counseling and quit-line referral for parents who smoke’, Academic Pediatrics 14(5), pp. 478-484 (DOI: 10.1016/j.acap.2014.03.017).
Sharpe, R. A., et al., 2015, ‘Indoor fungal diversity and asthma: a meta-analysis and systematic review of risk factors’, Journal of Allergy and Clinical Immunology 135(1), pp. 110-122 (DOI: 10.1016/j.jaci.2014.07.002).
Tainio, M., et al., 2021, ‘Air pollution, physical activity and health: a mapping review of the evidence’, Environment International 147, 105954 (DOI: 10.1016/j.envint.2020.105954).
EEA and WHO Europe et al. (eds.), 2003, Children’s health and environment: a review of evidence, Environmental Issue Report No 29/2002, European Environment Agency and World Health Organization Regional Office for Europe (https://www.eea.europa.eu/publications/environmental_issue_report_2002_29) accessed 5 April 2023.
Tham, R., et al., 2014, ‘Outdoor fungi and child asthma health service attendances’, Pediatric Allergy and Immunology 25(5), pp. 439-449 (DOI: 10.1111/pai.12257).
Thevenet, F., et al., 2018, ‘VOC uptakes on gypsum boards: sorption performances and impact on indoor air quality’, Building and Environment 137, pp. 138-146 (DOI: 10.1016/j.buildenv.2018.04.011).
Tomson, M., et al., 2021, ‘Green infrastructure for air quality improvement in street canyons’, Environment International146, 106288 (DOI: 10.1016/j.envint.2020.106288).
Trasande, L., et al., 2016, ‘Burden of disease and costs of exposure to endocrine disrupting chemicals in the European Union: an updated analysis’, Andrology 4(4), pp. 565-572 (DOI: 10.1111/andr.12178).
Tremper, A. H., et al., 2015, Impact of green screens on concentrations of particulate matter and oxides of nitrogen in near road environments, King’s College London, Environmental Research Group (https://www.londonair.org.uk/london/reports/GreenScreen_Report.pdf) accessed 5 April 2023.
Tremper, A. H. and Green, D. C., 2018, The impact of a green screen on concentrations of nitrogen dioxide at Bowes Primary School, Enfield, King’s College London, Environmental Research Group (https://www.londonair.org.uk/london/reports/Green_Screen_Enfield_Report_final.pdf) accessed 5 April 2023.
Turner, S., et al., 2020, ‘Associations between a smoke-free homes intervention and childhood admissions to hospital in Scotland: an interrupted time-series analysis of whole-population data’, The Lancet Public Health 5(9), pp. e493-e500 (DOI: 10.1016/S2468-2667(20)30178-X).
UBA, 2023, German Committee on Indoor Air Guide Values, Umweltbundesamt. (https://www.umweltbundesamt.de/en/gallery/guide-values-for-the-concentration-of-specific). Accessed 14 April 2023.
US EPA, 2015, Integrated science assessment (ISA) for nitrogen dioxide — health criteria, United States Environmental Protection Agency (https://www.epa.gov/isa/integrated-science-assessment-isa-nitrogen-dioxide-health-criteria) accessed 11 March 2022.
US EPA, 2017, Integrated science assessment (ISA) for sulfur oxides — health criteria, United States Environmental Protection Agency (https://www.epa.gov/isa/integrated-science-assessment-isa-sulfur-oxides-health-criteria) accessed 11 March 2022.
US EPA, 2019, Integrated science assessment (ISA) for particulate matter, United States Environmental Protection Agency (https://www.epa.gov/isa/integrated-science-assessment-isa-particulate-matter) accessed 11 March 2022.
US EPA, 2020, Integrated science assessment (ISA) for ozone and related photochemical oxidants, United States Environmental Protection Agency (https://www.epa.gov/isa/integrated-science-assessment-isa-ozone-and-related-photochemical-oxidants) accessed 11 March 2022.
US EPA, O., 2010, Integrated science assessment (ISA) for carbon monoxide, United States Environmental Protection Agency (https://www.epa.gov/isa/integrated-science-assessment-isa-carbon-monoxide) accessed 11 March 2022.
Valent, F., et al., 2004, ‘Burden of disease attributable to selected environmental factors and injury among children and adolescents in Europe’, The Lancet 363(9426), pp. 2032-2039 (DOI: 10.1016/S0140-6736(04)16452-0).
Vlaamse Regering, 2004, ‘Binnenmilieubesluit — Besluit van de Vlaamse Regering van 11 juni 2004 houdende maatregelen tot bestrijding van de gezondheidsrisico’s door verontreiniging van het binnenmilieu’ (https://www.zorg-en-gezondheid.be/binnenmilieubesluit-besluit-van-de-vlaamse-regering-van-11-juni-2004-houdende-maatregelen-tot) accessed 16 August 2022.
Wei, T., et al., 2021, ‘Exposure to outdoor air pollution at different periods and the risk of leukemia: a meta-analysis’, Environmental Science and Pollution Research International 28(27), pp. 35376-35391 (DOI: 10.1007/s11356-021-14053-8).
WHO, 2018, Air pollution and child health: prescribing clean air, World Health Organization (https://www.who.int/publications/i/item/WHO-CED-PHE-18-01) accessed 5 April 2023.
WHO, 2021a, Compendium of WHO and other UN guidance on health and environment, WHO/HEP/ECH/EHD/21.02, World Health Organization (https://apps.who.int/iris/rest/bitstreams/1365634/retrieve) accessed 14 February 2022.
WHO, 2021b, WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide, World Health Organization (https://apps.who.int/iris/handle/10665/345329) accessed 5 April 2023.
WHO, 2022, WHO guidelines for indoor air quality: dampness and mould, World Health Organization (https://www.who.int/publications-detail-redirect/9789289041683) accessed 30 August 2022.
WHO, 2023, ‘Maternal, newborn, child and adolescent health and ageing data portal’, World Health Organization (https://platform.who.int/data/maternal-newborn-child-adolescent-ageing) accessed 5 April 2023.
Wolfe, M. K., et al., 2021, ‘Impact of school location on children’s air pollution exposure’, Journal of Urban Affairs 43(8), pp. 1118-1134 (DOI: 10.1080/07352166.2020.1734013).
WHO Europe, 2009, Damp and mould: health risks, prevention and remedial actions, World Health Organization Regional Office for Europe (https://www.euro.who.int/__data/assets/pdf_file/0003/78636/Damp_Mould_Brochure.pdf) accessed 5 April 2023.
WHO Europe, 2022, Measures to reduce risks for children’s health from combined exposure to multiple chemicals in indoor air in public settings for children with a focus on schools, kindergartens and day-care centres: supplementary publication to the screening tool for assessment of health risks from combined exposure to multiple chemicals in indoor air in public settings for children, World Health Organization Regional Office for Europe (https://apps.who.int/iris/handle/10665/354225) accessed 5 April 2023.
Yan, W., et al., 2020, ‘The impact of prenatal exposure to PM2.5 on childhood asthma and wheezing: a meta-analysis of observational studies’, Environmental Science and Pollution Research Int 27(23), pp. 29280-29290 (DOI: 10.1007/s11356-020-09014-6).
Yang, B. Y., et al., 2020, ‘Ambient air pollution and diabetes: a systematic review and meta-analysis’, Environmental Research 180, 108817 (DOI: 10.1016/j.envres.2019.108817).
Yu, Z., et al., 2022, ‘Gestational exposure to ambient particulate matter and preterm birth: an updated systematic review and meta-analysis’, Environmental Research 212(Pt C), 113381 (DOI: 10.1016/j.envres.2022.113381).
Zhang, H., et al., 2021, ‘Ambient air pollution and stillbirth: an updated systematic review and meta-analysis of epidemiological studies’, Environmental Pollution 278, 116752 (DOI: 10.1016/j.envpol.2021.116752).
Zheng, X. Y., et al., 2021, ‘Short-term exposure to ozone, nitrogen dioxide, and sulphur dioxide and emergency department visits and hospital admissions due to asthma: a systematic review and meta-analysis’, Environment International 150, 106435 (DOI: 10.1016/j.envint.2021.106435).
Zhu, W., et al., 2022, ‘The correlation between chronic exposure to particulate matter and spontaneous abortion: a meta-analysis’, Chemosphere 286(Pt 2), 131802 (DOI: 10.1016/j.chemosphere.2021.131802).
Ziou, M., et al., 2022, ‘Outdoor particulate matter exposure and upper respiratory tract infections in children and adolescents: a systematic review and meta-analysis’, Environmental Research 210, 112969 (DOI: 10.1016/j.envres.2022.112969).
Zu, K., et al., 2018, ‘Critical review of long-term ozone exposure and asthma development’, Inhalation Toxicology 30(3), pp. 99-113 (DOI: 10.1080/08958378.2018.1455772).

Document Actions
Share with others